Introduction: Type 2 diabetes is a significant global health concern, necessitating a thorough understanding of its metabolic processes for effective management. The role of glycated hemoglobin (HbA1c) is crucial, particularly in relation to lipid biomarkers, which warrants exploration to enhance early detection and prediction of diabetes risk in individuals. Objective: This study aimed to explore the associations between HbA1c and lipid biomarkers in diabetic and non-diabetic individuals and to identify key predictors of type 2 diabetes. Methods: A case-control study at the Central Hospital of Yaoundé involved 70 type 2 diabetes patients and 67 non-diabetic controls. Data on sociodemographic characteristics, blood pressure, and biochemical markers were analyzed using Principal Component Analysis, Spearman’s rank correlation, multivariate linear and logistic regressions, and LASSO logistic regression. Results: The findings demonstrate a differential relationship between HbA1c and HDL-cholesterol in diabetic and non-diabetic groups, with diabetics exhibiting distinct metabolic profiles illustrated with lipid levels more closely associated with obesity and inflammation. Among non-diabetic participants, HbA1c was significantly inversely associated with HDL cholesterol (r = -0.337, p = 0.006), while in diabetic participants, it was positively associated with fasting blood glucose (r = 0.277, p = 0.023). Multivariate linear models indicated that the negative association between HDL cholesterol and HbA1c in non-diabetic participants was glycemia-independent. The predictive model identified HbA1c, age, education level, marital status, HDL cholesterol, and C-reactive protein as key predictors of type 2 diabetes, demonstrating high performance with a pseudo-R-square value of 0.8517, sensitivity of 94.03%, specificity of 96.97%, and an AUC of 0.9948. Notably, the adjusted cutoff value of HbA1c was 7.59%, significantly higher than the unadjusted value of 6.05% (t = 13.52, p = 0.001). Conclusion: The study shows a distinct relationship between HbA1c and HDL-cholesterol, linking diabetes to lipid levels, obesity, and inflammation. These findings emphasize context-specific HbA1c interpretation for better diabetes risk prediction and management.
| Published in | International Journal of Diabetes and Endocrinology (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijde.20251001.11 |
| Page(s) | 1-16 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
HbA1c, Lipid Biomarkers, Predictive Model, Sociodemographic Factors, Type 2 Diabetes
Variables | Diabetic (n=70) | Non-diabetic (n=67) | Total | p-value |
|---|---|---|---|---|
Sex – N (%) | ||||
Male | 22 (31.4) | 18 (26.9) | 40 (29.2) | 0.557 |
Female | 48 (68.6) | 49 (73.1) | 97 (70.8) | |
Age (years) – Mean (SD) | 56.8 (12.6) | 33.4 (11.9) | 45.4 (17.0) | < 0.001 |
Education – N (%) | ||||
None | 3 (4.3) | 0 (0.0) | 3 (2.2) | < 0.001 |
Primary | 19 (27.1) | 5 (7.5) | 24 (17.5) | |
Secondary | 34 (48.6) | 11 (16.4) | 45 (32.8) | |
Post-graduate | 14 (20.0) | 51 (76.1) | 65 (47.5) | |
Marital status – N (%) | ||||
Single | 7 (10.0) | 47 (70.1) | 54 (39.4) | < 0.001 |
Widow | 16 (22.9) | 3 (4.5) | 19 (13.9) | |
Divorced | 2 (2.9) | 2 (3.0) | 4 (2.9) | |
Married | 45 (64.3) | 15 (22.4) | 60 (43.8) | |
Profession – N (%) | ||||
Student | 0 (0.0) | 34 (50.7) | 34 (24.8) | < 0.001 |
Housewife | 17 (24.3) | 2 (3.0) | 19 (13.9) | |
Trader | 3 (4.5) | 12 (17.1) | 15 (10.9) | |
Teacher | 4 (6.0) | 3 (4.3) | 7 (5.1) | |
Tailor | 1 (1.5) | 3 (4.3) | 4 (2.9) | |
Retired | 3 (4.5) | 17 (24.3) | 20 (14.6) | |
Other | 20 (29.9) | 18 (25.7) | 38 (27.7) | |
Body mass index – N (%) | ||||
Underweight | 1 (1.4) | 2 (3.0) | 3 (2.2) | 0.233 |
Normal weight | 14 (20.0) | 23 (34.3) | 37 (27.0) | |
Overweight | 33 (47.1) | 24 (35.8) | 57 (41.6) | |
Obese | 22 (31.4) | 18 (26.9) | 40 (29.2) | |
Systolic blood pressure – Mean (SD) | 135.4 (19.8) | 121.4 (13.7) | 128 (18) | < 0.001 |
Diastolic blood pressure – Mean (SD) | 84.2 (11.9) | 80.5 (10.7) | 82 (11) | 0.057 |
Variable | HDL-cholesterol | LDL-cholesterol | Triglycerides | Total cholesterol | TChol/HDL Ratio | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Adj. β | p-value | Adj. β | p-value | Adj. β | p-value | Adj. β | p-value | Adj. β | p-value | |
HbA1c (%) | -1.03 | 0.013* | 0.11 | 0.770 | 0.31 | 0.453 | -0.48 | 0.356 | 1.53 | 0.331 |
Diabetes status | ||||||||||
Yes | 5.34 | 0.043* | -2.16 | 0.370 | -4.07 | 0.144 | 1.59 | 0.611 | -13.67 | 0.139 |
No | 1 | 1 | 1 | 1 | 1 | |||||
HbA1c_Diabetes status | 1.01 | 0.030* | -0.20 | 0.626 | -0.70 | 0.146 | 0.58 | 0.315 | -2.14 | 0.191 |
Age (years) | -0.02 | 0.405 | -0.03 | 0.212 | -0.00 | 0.977 | -0.03 | 0.306 | 0.01 | 0.870 |
Sex | ||||||||||
Female | 0.42 | 0.375 | 0.02 | 0.965 | -0.04 | 0.930 | 0.07 | 0.910 | 0.46 | 0.603 |
Male | 1 | 1 | 1 | 1 | 1 | |||||
BMI | 0.07 | 0.169 | 0.14 | 0.010* | -0.03 | 0.549 | 0.22 | 0.004* | 0.08 | 0.156 |
Hypertension status | ||||||||||
Elevated blood pressure | -0.28 | 0.621 | -0.44 | 0.444 | -0.50 | 0.463 | -0.17 | 0.823 | -0.93 | 0.395 |
Hypertension stage 1 | 1.21 | 0.220 | -0.63 | 0.483 | -0.82 | 0.369 | -21.09 | 0.999 | -19.48 | 0.999 |
Hypertension stage 2 | -0.39 | 0.446 | -0.74 | 0.154 | -0.03 | 0.960 | -0.37 | 0.576 | -0.40 | 0.668 |
Normal | 1 | 1 | 1 | 1 | 1 | |||||
C-reactive protein (mg/dl) | -0.05 | 0.158 | -0.02 | 0.262 | 0.03 | 0.465 | -0.01 | 0.707 | 0.02 | 0.326 |
Education | ||||||||||
Primary | 2.12 | 0.152 | 0.98 | 0.510 | -0.40 | 0.801 | -0.06 | 0.974 | 0.41 | 0.834 |
Secondary | 1.05 | 0.131 | -0.24 | 0.712 | 0.60 | 0.495 | 0.14 | 0.862 | -0.55 | 0.674 |
Post-secondary | 0.94 | 0.096 | -0.31 | 0.561 | 0.14 | 0.829 | 0.03 | 0.965 | -0.23 | 0.821 |
None | 1 | 1 | 1 | 1 | 1 | |||||
Marital status | ||||||||||
Widow | 0.87 | 0.140 | 1.06 | 0.070 | -1.31 | 0.056 | 1.82 | 0.017* | -0.01 | 0.990 |
Divorced | 0.48 | 0.501 | 0.72 | 0.317 | -1.27 | 0.119 | 1.99 | 0.029* | 0.97 | 0.413 |
Married | 1.41 | 0.266 | -0.08 | 0.945 | -1.22 | 0.358 | 0.76 | 0.584 | -19.99 | 0.999 |
Single | 1 | 1 | 1 | 1 | 1 | |||||
Variables | Spearman correlation | p-value |
|---|---|---|
All participants | ||
Fasting blood glucose | 0.667 | < 0.001* |
Total cholesterol | 0.049 | 0.576 |
HDL-cholesterol | -0.162 | 0.063 |
Total cholesterol/HDL ratio | 0.181 | 0.037* |
LDL-cholesterol | 0.026 | 0.767 |
Triglycerides | 0.210 | 0.006* |
Non-Diabetic participants | ||
Fasting blood glucose | -0.005 | 0.970 |
Total cholesterol | -0.044 | 0.723 |
HDL-cholesterol | -0.337 | 0.006* |
Total cholesterol/HDL ratio | 0.221 | 0.075 |
LDL-cholesterol | 0.066 | 0.596 |
Triglycerides | -0.005 | 0.965 |
Diabetic participants | ||
Fasting blood glucose | 0.277 | 0.023* |
Total cholesterol | -0.041 | 0.744 |
HDL-cholesterol | -0.070 | 0.574 |
Total cholesterol/HDL ratio | 0.094 | 0.450 |
LDL-cholesterol | -0.011 | 0.932 |
Triglycerides | 0.110 | 0.374 |
Variable | Model 1 (Unadjusted) | Model 2 (Adjusted for glycemia) | Model 3 (Fully adjusted) | ||||||
|---|---|---|---|---|---|---|---|---|---|
β | 95%CI | p-value | Adj. β | 95%CI | p-value | Adj. β | 95%CI | p-value | |
Triglycerides | 0.91 | 0.18, 1.64 | 0.015* | 0.33 | -0.32, 0.97 | 0.317 | -0.01 | -0.63, 0.60 | 0.964 |
Fasting blood glucose | 1.14 | 0.83, 1.46 | <0.001* | 0.78 | 0.45, 1.10 | <0.001* | |||
CRP | 0.00 | -0.01, 0.02 | 0.868 | ||||||
BMI | -0.04 | -0.09, 0.00 | 0.064 | ||||||
Sex | -0.20 | -0.71, 0.31 | 0.443 | ||||||
Age | 0.02 | 0.01, 0.04 | 0.009* | ||||||
Education | -0.12 | -0.47, 0.23 | 0.498 | ||||||
Marital status | 0.21 | 0.02, 0.40 | 0.027* | ||||||
Hypertension status | 0.16 | -0.05, 0.38 | 0.129 | ||||||
Variable | Model 1 (Unadjusted) | Model 2 (Adjusted for glycemia) | Model 3 (Fully adjusted) | ||||||
|---|---|---|---|---|---|---|---|---|---|
β | 95%CI | p-value | Adj. β | 95%CI | p-value | Adj. β | 95%CI | p-value | |
HDL-cholesterol | -3.08 | -5.45, -0.72 | 0.011* | -3.15 | -5.56, -0.75 | 0.011* | -2.97 | -5.86, -0.09 | 0.044* |
Fasting blood glucose | -0.38 | -2.30, 1.54 | 0.693 | -0.25 | -2.46, 1.96 | 0.820 | |||
CRP | -0.04 | -0.09, 0.01 | 0.100 | ||||||
BMI | 0.02 | -0.02, 0.06 | 0.356 | ||||||
Sex | -0.12 | -0.53, 0.28 | 0.542 | ||||||
Age | -0.01 | -0.04, 0.02 | 0.446 | ||||||
Education | -0.07 | -0.52, 0.38 | 0.745 | ||||||
Marital status | 0.05 | -0.15, 0.25 | 0.628 | ||||||
Hypertension status | -0.05 | -0.23, 0.13 | 0.606 | ||||||
Variable | Coefficient | Odds ratio | p-value | ||
|---|---|---|---|---|---|
Value | 95% CI | Value | 95%CI | ||
HbA1c | 3.55 | 1.62, 5.48 | 34.94 | 5.06, 241.27 | < 0.001 |
Age | 0.20 | 0.05, 0.35 | 1.22 | 1.05, 1.41 | 0.009 |
Education level | -0.07 | -1.66, 1.52 | 0.93 | 0.19, 4.58 | 0.930 |
Marital status | 0.17 | -0.79, 1.13 | 1.19 | 0.45, 3.10 | 0.726 |
HDL-cholesterol | 6.19 | -4.69, 17.07 | 487.36 | 0.01, 2.58 107 | 0.265 |
C-reactive protein | 0.07 | -0.11, 0.25 | 1.07 | 0.90, 1.28 | 0.428 |
Constant | -33.58 | -54.33, -12.82 | 2.62 10-15 | 2.53 10-24, 2.7 10-6 | 0.002 |
Metric | Value |
|---|---|
Pseudo R2 | 0.8517 |
Log-likelihood | - 13.67 |
Sensitivity | 94.03% |
Specificity | 96.97% |
Positive predictive value | 96.92% |
Negative predictive value | 94.12% |
Area under the curve (AUC) | 0.9948 |
Mean Squared Error (MSE) | 0.03052795 |
Root Mean Squared Error (RMSE) | 0.0616976 |
Mean Absolute Error (MAE) | 0.0616976 |
Accuracy | 95.49% |
Akaike Information Criterion (AIC) | 41.34 |
Bayesian Information Criterion (BIC) | 61.58 |
T2D | Type 2 Diabetes |
IDF | International Diabetes Federation |
HbA1c | Glycated Hemoglobin |
FBG | Fasting Blood Glucose |
TG | Triglycerides |
HDL | High-density Lipoprotein |
BMI | Body Mass Index |
BP | Blood Pressure |
SBP | Systolic Blood Pressure |
DBP | Diastolic Blood Pressure |
WHO | World Health Organization |
GOD-PAP | The Glucose Oxidase 4-aminoantipyrine Peroxidase |
EDTA | Ethylene Diamine Tetraacetate |
CRP | C-reactive Protein |
CHOD-PAD | Cholesterol Oxidase 4-aminoantipyrine Peroxidase |
CHOD-POD | Cholesterol Oxidase Peroxidase |
GOD-PAP | Glycerophosphate Oxidase Peroxidase |
LDL | Low-density Lipoprotein |
TC | Total Cholesterol |
AUC | Area Under the Curve |
MSE | Mean Squared Error |
RMSE | Root Mean Squared Error |
MAE | Mean Absolute Error |
AIC | Akaike Information Criterion |
BIC | Bayesian Information Criterion |
ROC | Receiver Operating Characteristic Curve |
PCA | Principal Component Analysis |
PC | Principal Component |
| [1] | American Diabetes Association, 6. Glycemic Targets: Standards of Medical Care in Diabetes—2021, Diabetes Care. 2021, 44 (Supplement 1), S73-S84. |
| [2] |
International Diabetes Federation, IDF Diabetes Atlas, 10th edn. Brussels, Belgium: 2021. Available from:
https://www.diabetesatlas.org (accessed September 20, 2024). |
| [3] | Selvin, E., Steffes, M. W., Zhu, H., Matsushita, K., Wagenknecht, L., Pankow, J., Coresh, J., & Brancati, F. L., Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults, N Engl J Med. 2010, 362(9), 800-811. |
| [4] | Nathan, D. M., Kuenen, J., Borg, R., Zheng, H., Schoenfeld, D., Heine, R. J., & A1c-Derived Average Glucose Study Group, Translating the A1C assay into estimated average glucose values, Diabetes Care. 2008, 31(8), 1473-1478. |
| [5] | Ram, Y., Xu, Y., Cheng, A., Dunn, T., & Ajjan, R. A., Variation in the relationship between fasting glucose and HbA1c: implications for the diagnosis of diabetes in different age and ethnic groups, BMJ Open Diabetes Res Care. 2024, 12(2), e003470. |
| [6] | Xue, T., Jiang, M., Liu, Y., Hu, Q., Zhu, B., Hu, J., Guo, W., Wu, X., Xiong, Y., Shi, X., Zhang, X., Han, X., Li, W., Tong, R., & Long, E., Predicting three-month fasting blood glucose and glycated hemoglobin changes in patients with type 2 diabetes mellitus based on multiple machine learning algorithms, Sci Rep. 2023, 13, 16437. |
| [7] | Ngoufack, J. O., Mbouemboue, O. P., Touko, A. M., Haman, H. S., Amanissa, P. D., Amvene, M. J., & Tamanji, M. T., Relationship between HbA1c level and Cardiometabolic Markers in Diabetic patients from Ngaoundere, Health Sci. Dis. 2018, 19(3), 1-7. |
| [8] | Sherwani, S. I., Khan, H. A., Ekhzaimy, A., Masood, A., & Sakharkar, M. K., Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients, Biomarker Insights. 2016, 11. |
| [9] | Ghazanfari, Z., Haghdoost, A. A., Alizadeh, S. M., Atapour, J., & Zolala, F., A Comparison of HbA1c and Fasting Blood Sugar Tests in General Population, Int J Prev Med. 2010, 1(3), 187-194. |
| [10] | Haase, C. L., Tybjærg-Hansen, A., Nordestgaard, B. G., & Frikke-Schmidt, R., HDL Cholesterol and Risk of Type 2 Diabetes: A Mendelian Randomization Study, Diabetes. 2015, 64(9), 3328–3333. |
| [11] | Fanni, G., Rosato, R., Gentile, L., Anselmino, M., Frea, S., Ponzo, V., Pellegrini, M., Broglio, F., Pivari, F., De Ferrari, G. M., Ghigo, E., & Bo, S., Is HDL cholesterol protective in patients with type 2 diabetes? A retrospective population-based cohort study, J Transl Med. 2020, 18(1), 189. |
| [12] | Femlak, M., Gluba-Brzózka, A., Ciałkowska-Rysz, A., et al., The role and function of HDL in patients with diabetes mellitus and the related cardiovascular risk, Lipids Health Dis. 2017, 16, 207. |
| [13] | Sabanayagam, C., Khoo, E. Y., Lye, W. K., Ikram, M. K., Lamoureux, E. L., Cheng, C. Y., Tan, M. L., Salim, A., Lee, J., Lim, S. C., Tavintharan, S., Thai, A. C., Heng, D., Ma, M. A., Tai, S., Wong, E. S., & Wong, T. Y. T. Y., Diagnosis of diabetes mellitus using HbA1c in Asians: relationship between HbA1c and retinopathy in a multiethnic Asian population, J Clin Endocrinol Metab. 2015, 100(2), 689-696. |
| [14] |
Diabetes UK, Diagnostic criteria for diabetes, 2023. Available from:
https://www.diabetes.org.uk/for-professionals/improving-care/clinical-recommendations-for-professionals/diagnosisongoing-management-monitoring/new_diagnostic_criteria_for_diabetes (accessed 22 September 2024). |
| [15] | Karnchanasorn, K., Huang, J., Ou, H.-Y., Feng, W., Chuang, L.-M., Chiu, K. C., & Samoa, R., Comparison of the Current Diagnostic Criterion of HbA1c with Fasting and 2-Hour Plasma Glucose Concentration, Journal of Diabetes Research. 2016. |
| [16] | Wang, B., Liu, M. C., Li, X. Y., Liu, X. H., Feng, Q. X., Lu, L., Zhu, Z., Liu, Y. S., Zhao, W., & Gao, Z. N., Cutoff Point of HbA1c for Diagnosis of Diabetes Mellitus in Chinese Individuals, PLoS One. 2016, 11(11), e0166597. |
| [17] | Charan, J., Biswas, T., How to Calculate Sample Size for Different Study Designs in Medical Research? Indian Journal Psychological Medicine. 2013, 35(2), 121–126. |
| [18] | Bigna, J. J., Nansseu, J. R., Katte, J. C., & Noubiap, J. J., Prevalence of prediabetes and diabetes mellitus among adults residing in Cameroon: A systematic review and meta-analysis, Diabetes Res Clin Pract. 2018, 137, 109-118. |
| [19] | Whelton, P. K., Carey, R. M., Aronow, W. S., et al., 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, Journal of the American College of Cardiology. 2018, 71(19), 122. |
| [20] | World Health Organization, WHO guidelines on drawing blood: best practices in phlebotomy, Geneva: World Health Organization, 2010. |
| [21] | Trinder, P., Determination of glucose in blood using glucose oxidase with an alternative oxygen acceptor, Annals of Clinical Biochemistry. 1969, 6(1), 24-27. |
| [22] | Friedewald, W. T., Levy, R. I., & Fredrickson, D. S., Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge, Clinical Chemistry. 1972, 18(6), 499-502. |
| [23] | Expert Panel on Detection, Evaluation, Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III), JAMA. 2001, 285(19), 2486-2497. |
| [24] | Wisniewski, A., DeLouize, A. M., Walker, T., Chatterji, S., Naidoo, N., Kowal, P., & Snodgrass, J. J., Sustained metabolic dysregulation and the emergence of diabetes: associations between HbA1c and metabolic syndrome components in Tunisian diabetic and nondiabetic groups, J Physiol Anthropol. 2024, 43, 18. |
| [25] | Chait, A., & den Hartigh, L. J., Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease, Front. Cardiovasc. Med. 2020, 7, 22. |
| [26] | Naqvi, S., Naveed, S., Ali, Z., Ahmad, S. M., Khan, R. Asadullah, Raj, H., Shariff, S., Rupareliya, C., Zahra, F., & Khan, S., Correlation between Glycated Hemoglobin and Triglyceride Level in Type 2 Diabetes Mellitus, Cureus. 2017, 9(6), e1347. |
| [27] | Sinning, C., Makarova, N., Völzke, H., Schnabel, R. B., Ojeda, F., Dörr, M., Felix, S. B., Koenig, W., Peters, A., Rathmann, W., Schöttker, B., Brenner, H., Veronesi, G., Cesana, G., Brambilla, P., Palosaari, T., Kuulasmaa, K., Njølstad, I., Mathiesen, E. B., Wilsgaard, T., Blankenberg, S., Söderberg, S., Ferrario, M. M., & Thorand, B., Association of glycated hemoglobin A1c levels with cardiovascular outcomes in the general population: results from the BiomarCaRE (Biomarker for Cardiovascular Risk Assessment in Europe) consortium, Cardiovasc Diabetol. 2021, 20, 223. |
| [28] | Sharahili, A. Y., Mir, S. A., ALDosari, S., Manzar, M. D., Alshehri, B., Al Othaim, A., Alghofaili, F., Madkhali, Y., Albenasy, K. S., & Alotaibi, J. S., Correlation of HbA1c Level with Lipid Profile in Type 2 Diabetes Mellitus Patients Visiting a Primary Healthcare Center in Jeddah City, Saudi Arabia: A Retrospective Cross-Sectional Study, Diseases. 2023, 11(4), 154. |
| [29] | Zheng, D., Dou, J., Liu, G., Pan, Y., Yan, Y., Liu, F., Gaisano, H. Y., Lu, J., & He, Y., Association Between Triglyceride Level and Glycemic Control Among Insulin-Treated Patients With Type 2 Diabetes, The Journal of Clinical Endocrinology & Metabolism. 2019, 104(4), 1211–1220. |
| [30] | Rodriguez-Gutierrez, R., Mancillas-Adame, L. G., Rodríguez-Tamez, G., Diaz Gonzalez-Colmenero, A., Solis-Pacheco, R. C., Elizondo-Plazas, A. S., Santos-Santillana, K. M., Gonzalez-Sariñana, L., Gonzalez-Nava, V., & Gonzalez-Gonzalez, J. G., Hypertriglyceridemia and Its Association with HbA1c Test: A Prospective In Vivo Controlled Study, Int J Endocrinol. 2019. |
| [31] | Huang, R., Yan, L., & Lei, Y., The relationship between high-density lipoprotein cholesterol (HDL-C) and glycosylated hemoglobin in diabetic patients aged 20 or above: a cross-sectional study, BMC Endocr Disord. 2021, 21, 198. |
| [32] | Gatti, A., Maranghi, M., Bacci, S., Carallo, C., Gnasso, A., Mandosi, E., Fallarino, M., Morano, S., Trischitta, V., & Filetti, S., Poor glycemic control is an independent risk factor for low HDL cholesterol in patients with type 2 diabetes, Diabetes Care. 2009, 32(8), 1550-1552. |
| [33] | Yan, Z., Xu, Y., Li, K., & Liu, L., Association between high-density lipoprotein cholesterol and type 2 diabetes mellitus: dual evidence from NHANES database and Mendelian randomization analysis, Front. Endocrinol. 2024, 15, 1272314. |
| [34] | Zheng, F., Yan, L., Yang, Z., et al., HbA1c, diabetes and cognitive decline: the English Longitudinal Study of Ageing, Diabetologia. 2018, 61, 839–848. |
| [35] | Kyrou, I., Tsigos, C., Mavrogianni, C., Cardon, G., Van Stappen, V., Latomme, J., Kivelä, J., Wikström, K., Tsochev, K., Nanasi, A., Semanova, C., Mateo-Gallego, R., Lamiquiz-Moneo, I., Dafoulas, G., Timpel, P., Schwarz, P. E. H., Iotova, V., Tankova, T., Makrilakis, K., & Manios, Y. on behalf of the Feel4Diabetes-study Group, Sociodemographic and lifestyle-related risk factors for identifying vulnerable groups for type 2 diabetes: a narrative review with emphasis on data from Europe, BMC Endocr Disord. 2020, 20, Suppl 1, 134. |
| [36] | Zhou, H., & Qin, G., Nonparametric Covariate Adjustment for the Youden Index, in Applied Statistics in Biomedicine and Clinical Trials Design, Z. Chen, A. Liu, Y. Qu, L. Tang, N. Ting, and Y. Tsong, Eds. Cham: Springer, 2015. |
| [37] | Fan, J., Upadhye, S., & Worster, A., Understanding receiver operating characteristic (ROC) curves, Canadian Journal of Emergency Medicine. 2006, 8(1), 19-20. |
APA Style
Saha, B. U. F., Choumessi, A. T., Teta, I., Kenmoe, J. C., Latsap, D. N. T., et al. (2025). Association Between Glycated Hemoglobin and Lipid Biomarkers in Diabetic and Non-diabetic Populations for Type 2 Diabetes Detection. International Journal of Diabetes and Endocrinology, 10(1), 1-16. https://doi.org/10.11648/j.ijde.20251001.11
ACS Style
Saha, B. U. F.; Choumessi, A. T.; Teta, I.; Kenmoe, J. C.; Latsap, D. N. T., et al. Association Between Glycated Hemoglobin and Lipid Biomarkers in Diabetic and Non-diabetic Populations for Type 2 Diabetes Detection. Int. J. Diabetes Endocrinol. 2025, 10(1), 1-16. doi: 10.11648/j.ijde.20251001.11
AMA Style
Saha BUF, Choumessi AT, Teta I, Kenmoe JC, Latsap DNT, et al. Association Between Glycated Hemoglobin and Lipid Biomarkers in Diabetic and Non-diabetic Populations for Type 2 Diabetes Detection. Int J Diabetes Endocrinol. 2025;10(1):1-16. doi: 10.11648/j.ijde.20251001.11
@article{10.11648/j.ijde.20251001.11,
author = {Brice Ulrich Foudjo Saha and Aphrodite Tchewonpi Choumessi and Ismael Teta and Jonathan Chefang Kenmoe and Daliane Naomi Tezempa Latsap and Lifoter Kenneth Navti and Edouard Akono Nantia},
title = {Association Between Glycated Hemoglobin and Lipid Biomarkers in Diabetic and Non-diabetic Populations for Type 2 Diabetes Detection},
journal = {International Journal of Diabetes and Endocrinology},
volume = {10},
number = {1},
pages = {1-16},
doi = {10.11648/j.ijde.20251001.11},
url = {https://doi.org/10.11648/j.ijde.20251001.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijde.20251001.11},
abstract = {Introduction: Type 2 diabetes is a significant global health concern, necessitating a thorough understanding of its metabolic processes for effective management. The role of glycated hemoglobin (HbA1c) is crucial, particularly in relation to lipid biomarkers, which warrants exploration to enhance early detection and prediction of diabetes risk in individuals. Objective: This study aimed to explore the associations between HbA1c and lipid biomarkers in diabetic and non-diabetic individuals and to identify key predictors of type 2 diabetes. Methods: A case-control study at the Central Hospital of Yaoundé involved 70 type 2 diabetes patients and 67 non-diabetic controls. Data on sociodemographic characteristics, blood pressure, and biochemical markers were analyzed using Principal Component Analysis, Spearman’s rank correlation, multivariate linear and logistic regressions, and LASSO logistic regression. Results: The findings demonstrate a differential relationship between HbA1c and HDL-cholesterol in diabetic and non-diabetic groups, with diabetics exhibiting distinct metabolic profiles illustrated with lipid levels more closely associated with obesity and inflammation. Among non-diabetic participants, HbA1c was significantly inversely associated with HDL cholesterol (r = -0.337, p = 0.006), while in diabetic participants, it was positively associated with fasting blood glucose (r = 0.277, p = 0.023). Multivariate linear models indicated that the negative association between HDL cholesterol and HbA1c in non-diabetic participants was glycemia-independent. The predictive model identified HbA1c, age, education level, marital status, HDL cholesterol, and C-reactive protein as key predictors of type 2 diabetes, demonstrating high performance with a pseudo-R-square value of 0.8517, sensitivity of 94.03%, specificity of 96.97%, and an AUC of 0.9948. Notably, the adjusted cutoff value of HbA1c was 7.59%, significantly higher than the unadjusted value of 6.05% (t = 13.52, p = 0.001). Conclusion: The study shows a distinct relationship between HbA1c and HDL-cholesterol, linking diabetes to lipid levels, obesity, and inflammation. These findings emphasize context-specific HbA1c interpretation for better diabetes risk prediction and management.},
year = {2025}
}
TY - JOUR T1 - Association Between Glycated Hemoglobin and Lipid Biomarkers in Diabetic and Non-diabetic Populations for Type 2 Diabetes Detection AU - Brice Ulrich Foudjo Saha AU - Aphrodite Tchewonpi Choumessi AU - Ismael Teta AU - Jonathan Chefang Kenmoe AU - Daliane Naomi Tezempa Latsap AU - Lifoter Kenneth Navti AU - Edouard Akono Nantia Y1 - 2025/02/10 PY - 2025 N1 - https://doi.org/10.11648/j.ijde.20251001.11 DO - 10.11648/j.ijde.20251001.11 T2 - International Journal of Diabetes and Endocrinology JF - International Journal of Diabetes and Endocrinology JO - International Journal of Diabetes and Endocrinology SP - 1 EP - 16 PB - Science Publishing Group SN - 2640-1371 UR - https://doi.org/10.11648/j.ijde.20251001.11 AB - Introduction: Type 2 diabetes is a significant global health concern, necessitating a thorough understanding of its metabolic processes for effective management. The role of glycated hemoglobin (HbA1c) is crucial, particularly in relation to lipid biomarkers, which warrants exploration to enhance early detection and prediction of diabetes risk in individuals. Objective: This study aimed to explore the associations between HbA1c and lipid biomarkers in diabetic and non-diabetic individuals and to identify key predictors of type 2 diabetes. Methods: A case-control study at the Central Hospital of Yaoundé involved 70 type 2 diabetes patients and 67 non-diabetic controls. Data on sociodemographic characteristics, blood pressure, and biochemical markers were analyzed using Principal Component Analysis, Spearman’s rank correlation, multivariate linear and logistic regressions, and LASSO logistic regression. Results: The findings demonstrate a differential relationship between HbA1c and HDL-cholesterol in diabetic and non-diabetic groups, with diabetics exhibiting distinct metabolic profiles illustrated with lipid levels more closely associated with obesity and inflammation. Among non-diabetic participants, HbA1c was significantly inversely associated with HDL cholesterol (r = -0.337, p = 0.006), while in diabetic participants, it was positively associated with fasting blood glucose (r = 0.277, p = 0.023). Multivariate linear models indicated that the negative association between HDL cholesterol and HbA1c in non-diabetic participants was glycemia-independent. The predictive model identified HbA1c, age, education level, marital status, HDL cholesterol, and C-reactive protein as key predictors of type 2 diabetes, demonstrating high performance with a pseudo-R-square value of 0.8517, sensitivity of 94.03%, specificity of 96.97%, and an AUC of 0.9948. Notably, the adjusted cutoff value of HbA1c was 7.59%, significantly higher than the unadjusted value of 6.05% (t = 13.52, p = 0.001). Conclusion: The study shows a distinct relationship between HbA1c and HDL-cholesterol, linking diabetes to lipid levels, obesity, and inflammation. These findings emphasize context-specific HbA1c interpretation for better diabetes risk prediction and management. VL - 10 IS - 1 ER -
Department of Biochemistry, Faculty of Science, The University of Bamenda, Bambili, Cameroon
Department of Biochemistry, Faculty of Science, The University of Bamenda, Bambili, Cameroon
UNICEF Kenya Country Office, Nairobi, Kenya
Department of Biochemistry, Faculty of Science, The University of Bamenda, Bambili, Cameroon
School of Health Sciences, Catholic University of Central Africa, Yaoundé, Cameroon
Department of Biochemistry, Faculty of Science, The University of Bamenda, Bambili, Cameroon
Department of Biochemistry, Faculty of Science, The University of Bamenda, Bambili, Cameroon
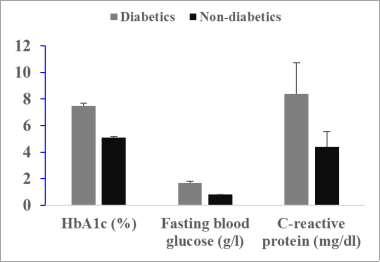
Figure 1. Distribution of HbA1c, fasting blood glucose, and C-reactive protein among diabetic and non-diabetic participants.
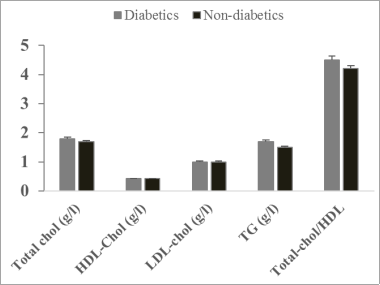
Figure 2. Lipid profile markers among diabetic and non-diabetic participants.
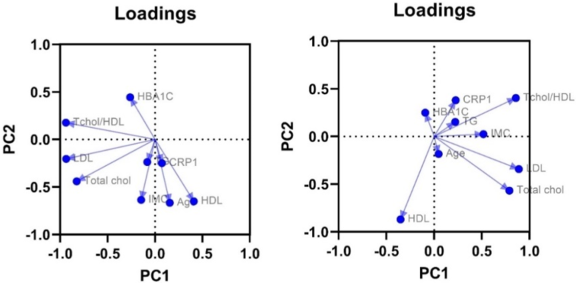
Figure 3. Loading plots of metabolic profiles of non-diabetic participants (on the left) and diabetic participants (on the right).
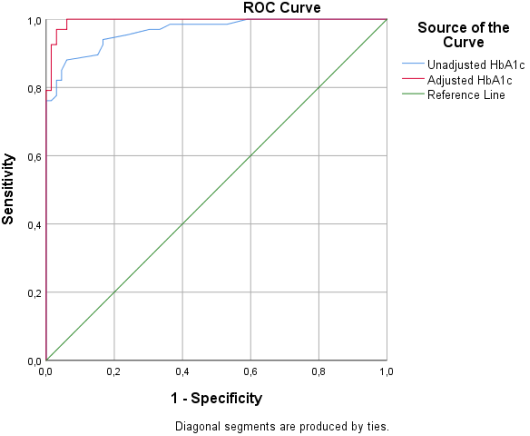
Figure 4. ROC curve of unadjusted and adjusted HbA1c.

