Abstract
Background: Although there are several clinical studies available regarding the management of Type 2 diabetes mellitus (T2DM), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the drivers of poor glycemic control, gaps in early screening, treatment choices, use of fixed-dose combinations (FDCs) of dapagliflozin, glimepiride, and metformin, safety considerations, and perceived glycemic outcomes in T2DM. Methodology: This cross-sectional study was carried out among 1,300 Indian clinical experts and utilized a multiple-response questionnaire to assess perspectives on poor glycemic control, screening gaps, and treatment patterns related to FDCs of dapagliflozin, glimepiride, and metformin. Responses were summarized using descriptive statistics and visualized using Microsoft Excel. Results: More than half of the participants (54.46%) identified a sedentary lifestyle and irregular follow-up visits as the principal contributors to poor glycemic control in routine clinical practice. A substantial majority (68.77%) indicated that inadequate awareness of early screening is the primary reason for elevated glycated hemoglobin (HbA1c) levels at diagnosis. Over half of the respondents (52.23%) perceived sulfonylureas to provide superior glycemic durability in clinical settings. Approximately 42% reported multiple factors, namely rapid and sustained glycemic control, reduced pill burden, and cost considerations, as key reasons for the early initiation of combination therapy. Nearly two-thirds of clinicians (63.46%) observed that patients with high baseline HbA1c levels (8–11%) experience the greatest benefit from the FDCs of dapagliflozin, glimepiride, and metformin. Conclusion: Uncontrolled T2DM is primarily driven by a sedentary lifestyle, poor follow-up, and low awareness of early screening. Clinicians favor sulfonylureas for glycemic durability and support early combination therapy for rapid control, improved adherence, and cost considerations. FDCs are perceived to delay insulin initiation, with patients presenting with high baseline HbA1c levels deriving the greatest benefit from the combination of dapagliflozin, glimepiride, and metformin.
Keywords
Uncontrolled T2DM, Glycaemic Durability, Early Combination Therapy, Fixed-dose Combinations, Treatment Adherence, Glimepiride
1. Introduction
Diabetes is a major global noncommunicable disease, with Type 2 diabetes mellitus (T2DM) accounting for nearly 90% of all cases.
| [1] | Al-Rifai RH, Aziz F. Prevalence of type 2 diabetes, prediabetes, and gestational diabetes mellitus in women of childbearing age in Middle East and North Africa, 2000-2017: protocol for two systematic reviews and meta-analyses. Syst Rev. 2018; 7(1): 96.
https://doi.org/10.1186/s13643-018-0763-0 |
| [2] | Yan S, Lu W, Zhou J, Guo X, Li J, Cheng H, et al. Aqueous extract of Scrophularia ningpoensis improves insulin sensitivity through AMPK-mediated inhibition of the NLRP3 inflammasome. Phytomedicine. 2022; 104: 154308.
https://doi.org/10.1016/j.phymed.2022.154308 |
| [3] | Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health. 2020; 10(1): 107–11. https://doi.org/10.2991/jegh.k.191028.001 |
[1-3]
India carries a substantial disease burden, with approximately 65.9 million affected individuals. Current recommendations advocate maintaining glycated hemoglobin (HbA1c) ≤7% for most nonpregnant adults to reduce the risk of microvascular and macrovascular complications.
| [3] | Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health. 2020; 10(1): 107–11. https://doi.org/10.2991/jegh.k.191028.001 |
| [4] | Dixit JV, Kulkarni RS, Badgujar SY. Diabetes Care in India: A Descriptive Study. Indian J Endocrinol Metab. 2021; 25(4): 342–7. https://doi.org/10.4103/ijem.ijem_260_21 |
[3, 4]
Despite established treatment guidelines and multiple therapeutic options, a considerable proportion of patients with T2DM fail to achieve recommended glycemic targets. Poor glycemic control remains associated with retinopathy, nephropathy, neuropathy, cardiovascular disease, and premature mortality. Because T2DM is progressive in nature, combination therapy is frequently considered when monotherapy fails to provide adequate glycemic control, with the aim of improving adherence, simplifying treatment regimens, and facilitating earlier attainment of therapeutic goals.
The combination of dapagliflozin, glimepiride, and metformin offers a multi-mechanistic approach to T2DM management.
| [6] | Sahay R, Gangwani D, Singh M, Gupta S, Kale N, Srivastava M, et al. Fixed dose combination of dapagliflozin, glimepiride and extended-release metformin tablets in patients with type 2 diabetes poorly controlled by metformin and glimepiride: A phase III, open label, randomized clinical study in India. Diabetes Obes Metab. 2025; 27(4): 2193–205.
https://doi.org/10.1111/dom.16218 |
[6]
Dapagliflozin, a sodium–glucose cotransporter-2 (SGLT2) inhibitor, lowers plasma glucose by increasing urinary glucose excretion.
Glimepiride improves glycemic control through stimulation of pancreatic insulin secretion,
| [8] | Basit A, Riaz M, Fawwad A. Glimepiride: evidence-based facts, trends, and observations (GIFTS). Vasc Health Risk Manag. 2012; 8: 463-72. https://doi.org/10.2147/HIV.S33194 |
[8]
whereas metformin reduces hepatic glucose production and improves insulin sensitivity.
| [9] | Dutta S, Shah RB, Singhal S, Dutta SB, Bansal S, Sinha S, et al. Metformin: A Review of Potential Mechanism and Therapeutic Utility Beyond Diabetes. Drug Des Devel Ther. 2023; 17: 1907-1932. https://doi.org/10.2147/DDDT.S409373 |
[9]
Although several studies have evaluated the efficacy and safety of dapagliflozin, glimepiride, and metformin, limited evidence exists regarding clinicians’ perspectives on their use in routine clinical practice. Therefore, this nationwide survey aimed to assess clinicians’ views on determinants of poor glycemic control, gaps in early screening, treatment decision-making, safety considerations, and perceived glycemic outcomes associated with contemporary fixed-dose combination therapy in T2DM management.
2. Materials and Methods
2.1. Study Settings
A cross-sectional study was conducted among clinicians involved in the management of T2DM across multiple clinical settings in India. Invitations and participant recruitment activities were initiated in March 2025, whereas questionnaire administration, survey completion, and data collection were conducted from June 2025 to December 2025. The study was performed in accordance with Bangalore Ethics, an Independent Ethics Committee (ECR/355/Indt/KA/2022), recognized by the Drug Controller General of India.
2.2. Study Participants
A convenient sampling technique was used, and an invitation was sent to professionals across India based on their expertise and experience in treating T2DM in the month of March 2025 for participation in this Indian survey. About 1,300 clinicians from major cities of all Indian states, representing the geographical distribution, shared their willingness to participate and provide necessary data. The primary survey included 22 core questions administered to 1300 clinicians, with an additional subset of 98 participants contributing to an extended survey in which 16 additional questions were included. Clinicians were instructed to complete the questionnaire independently without consulting colleagues. Written informed consent was obtained from each participant before the study began.
2.3. Study Procedure
A structured multiple-response questionnaire titled LEGACY (Oral Anti Diabetic Combination Therapy and Glycaemic Outcomes: Indian Expert Perspective Study) was used to capture clinician perspectives regarding poor glycemic control, screening gaps, treatment decision-making, and therapeutic practices related to fixed-dose combinations in routine clinical care. Reliability, as determined by a split-half test (coefficient alpha), was adequate but should be improved in future versions of the questionnaire. A study of criterion validity was undertaken to test the questionnaire and to develop methods of testing the validity of measures of Physicians' Perspectives. However, the extraneous variables in this include the clinician's experience, usage of the newer drugs, etc. The two criteria used were the doctors' perspectives from the clinical practice and the assessment of an external assessor and statistician. Clinicians had the option to skip questions as desired and were instructed to complete the survey independently, without peer consultation. Before participating in the survey, all respondents provided written informed consent.
2.4. Statistical Analysis
Survey responses were analyzed using descriptive statistical methods. Categorical variables were summarized using frequencies and percentages, while continuous variables, where applicable, were summarized using means and standard deviations. Because the primary objective of this survey was exploratory and descriptive, focusing on clinician perspectives and treatment patterns rather than hypothesis testing, inferential statistical analyses were not prespecified or performed.
Clinicians were permitted to skip questions where desired. Missing responses were handled using available-case analysis; percentages were calculated based on the number of respondents answering individual questions. No imputation procedures were applied. Data visualization, including charts and graphical summaries, was performed using Microsoft Excel 2013 (version 16.0.13901.20400).
3. Results
The survey comprised 1,300 experts, and more than half of the participants (54.46%) identified a sedentary lifestyle and irregular follow-up visits as the principal contributors to uncontrolled diabetes in routine clinical practice (
Table 1). Approximately 40% reported that 11–20% of newly diagnosed individuals with T2DM have HbA1c levels >9%. A substantial proportion (68.77%) indicated that inadequate awareness of early screening is the primary reason for elevated HbA1c at diagnosis (
Table 2).
Table 1. Distribution of responses to the reasons for uncontrolled diabetes in clinical practice.
Reasons | Response rate (n = 1300) |
Sedentary lifestyle | 27.46% |
Irregular follow-up visits to the doctor | 18.08% |
All of the above | 54.46% |
Table 2. Distribution of responses on the reasons for high HbA1c levels (at the time of diagnosis) in clinical practice.
Reasons | Response rate (n = 1300) |
Lack of awareness of early screening | 68.77% |
Lack of clinical infrastructure | 8.08% |
Poor access to health care facilities | 3.46% |
All of the above | 19.62% |
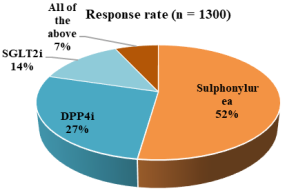
Nearly 43% of the experts preferred sulfonylureas as add-on therapy for patients with uncontrolled diabetes on stable metformin, and more than half (52.23%) perceived sulfonylureas to provide superior glycemic durability in clinical practice (
Figure 1). Regarding patient preference, about 35% reported that 21–30% of their patients with T2DM prefer glimepiride. Approximately 53% agreed that the cardiovascular outcomes trial (CVOT) supports the effectiveness and tolerability of glimepiride. Over half of the respondents (51.08%) observed a mean HbA1c reduction of 1.0–1.5% after 6 months of glimepiride–metformin therapy. Around 42% of respondents cited multiple factors, namely rapid and sustained glycemic control, reduced pill burden, and cost considerations, as reasons for the early initiation of combination therapy (
Table 3).
Table 3. Distribution of responses regarding views on the primary reasons for early initiation of combination therapy.
Primary reasons | Response rate (n = 1300) |
To have swift and sustained control | 34.92% |
To minimize the pill burden and improve compliance | 21.69% |
To minimize the cost burden | 1.62% |
All of the above | 41.69% |
Figure 1. Distribution of responses regarding drug classes associated with greater glycemic durability in clinical practice.
Around 42% strongly agreed, and 54% agreed that newer FDCs have delayed insulin initiation in patients with uncontrolled T2DM. A majority of clinicians (63.46%) reported that individuals with high baseline HbA1c levels (8–11%) derive the greatest benefit from the FDCs of dapagliflozin, glimepiride, and metformin (
Table 4). About 31% highlighted the complementary mechanisms of action of the dapagliflozin–glimepiride–metformin (ER) combination. Approximately 45% preferred this FDCs for 11–25% of high cardiovascular risk patients with uncontrolled T2DM. Nearly 48% reported a hypoglycemia incidence of 1–3% with the glimepiride–metformin–dapagliflozin regimen.
Table 4. Distribution of responses regarding patient subgroups that derive the maximum benefit from the FDC of dapagliflozin, glimepiride, and metformin in clinical practice.
Subgroups | Response rate (n = 1300) |
Newly diagnosed young T2DM individuals | 22.85% |
Diabetic individuals with high HbA1c levels (8 to 11%) | 63.46% |
Elderly diabetic individuals | 3.46% |
Long- standing elderly diabetic individuals | 2.85% |
All of the above | 7.31% |
Approximately 35% of the clinicians favored vildagliptin as the most commonly preferred dipeptidyl peptidase-4 inhibitor (DPP-4i) for patients with T2DM and cardiovascular risk. Nearly half of the participants (~47%) reported that CVOT evidence and demonstrated cardiovascular benefits are key drivers for prescribing sitagliptin in this population. About 32% indicated that disease duration and severity, glycemic variability, age, comorbidities, and renal function collectively inform decisions to prescribe glimepiride in combination with sitagliptin.
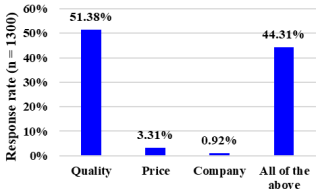
Approximately 52% reported using the newer single-pill combination of sitagliptin, glimepiride, and metformin in 11–20% of patients in clinical practice. About half (51%) considered quality the most important parameter when selecting a brand in clinical practice (
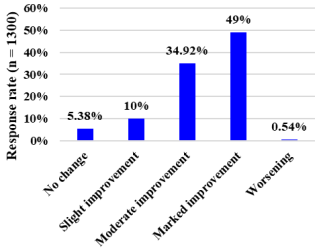
Figure 2). Regarding monitoring practices, 83% reported regularly monitoring patients for potential side effects or complications. Most participants (76.54%) reported no adverse drug reactions with glimepiride. On the 5-point global improvement scale, 49% rated glycemic control with glimepiride as showing marked improvement in routine clinical practice (
Figure 3).
Figure 2. Distribution of responses on the parameters considered most important when choosing a brand in clinical practice.
Figure 3. Distribution of responses on 5-point global improvement scale ratings of glycemic control with glimepiride in clinical practice.
Additional findings from the extended questionnaire involving 98 clinicians provided further insights into routine T2DM management practices. Approximately 53% reported that 11–25% of patients continued to have HbA1c >9% despite receiving oral antidiabetic therapy for more than one year. Nearly 45% of respondents identified older age, hypertension, smoking or tobacco use, and dyslipidemia collectively as the most common cardiovascular risk factors among newly diagnosed individuals with T2DM, while 59.18% frequently observed uncontrolled T2DM among patients aged 40–59 years. Around 49% of clinicians reported that 11–20% of patients with T2DM present with neuropathic pain, and approximately 48% indicated that 21–40% of patients progress to chronic kidney disease in routine clinical practice. Most respondents (77%) considered glycemic variability with the dapagliflozin, glimepiride, and metformin combination to be rare, whereas 58% observed an association between high glycemic variability and atherosclerotic cardiovascular disease in patients with diabetes. Additionally, nearly 36% of clinicians reported recommending self-monitoring of blood glucose for 51–75% of patients with T2DM as part of routine diabetes management.
4. Discussion
The findings of this survey highlight persistent gaps in glycemic control in routine T2DM management across India. The majority of clinicians attribute uncontrolled diabetes primarily to modifiable behavioral factors such as sedentary lifestyle and irregular follow-up, underscoring the need for stronger patient education, structured lifestyle counseling, and systematic follow-up strategies. Consistently, more than half of the participants identified sedentary behavior and irregular follow-up visits as the principal contributors to poor glycemic control in clinical practice.
These observations are supported by existing evidence. Lelyana Septia Damayanti emphasized the importance of reducing sedentary behavior in individuals with T2DM as a practical strategy to improve glycemic control and prevent long-term complications. Regular interruptions of prolonged sitting have been proposed as an effective non-pharmacological approach for optimizing blood glucose regulation.
| [10] | Damayanti LS. The impact of sedentary behavior on blood glucose levels in type 2 diabetes mellitus patients: A literature review. Journal of Evidence-based Nursing and Public Health. 2025; 2(1): 34–52.
https://doi.org/10.61511/jevnah.v2i1.2025.1735 |
[10]
Similarly, Bellettiere et al. demonstrated that higher levels of sedentary time, particularly when accumulated in prolonged uninterrupted bouts, are associated with increased odds of diabetes among older women. These findings reinforce the clinical relevance of minimizing sedentary time as an integral component of comprehensive diabetes management.
| [11] | Bellettiere J, Healy GN, LaMonte MJ, Kerr J, Evenson KR, Rillamas-Sun E, et al. Sedentary Behavior and Prevalent Diabetes in 6,166 Older Women: The Objective Physical Activity and Cardiovascular Health Study. J Gerontol A Biol Sci Med Sci. 2019; 74(3): 387–95. https://doi.org/10.1093/gerona/gly101 |
[11]
A large proportion of participants in the current survey identified poor awareness of early screening as the main reason for elevated HbA1c levels at the time of diagnosis. In a behavioral survey conducted in India, Ujjwal Halder found that only 13% of respondents had adequate knowledge of blood glucose levels, while 87% lacked a basic understanding of blood glucose concepts, risk factors, screening, and prevention. This limited awareness contributes to the delayed detection of diabetes, with many individuals remaining undiagnosed until symptoms or complications prompt medical attention, resulting in higher HbA1c levels at diagnosis than would be expected with earlier screening.
| [12] | Halder U. Diabetes as a pandemic: A sociological study on awareness, negligence and lifestyle at Howrah District. Int J Med Health Res. 2025; 11(6): 8-12. |
[12]
In a cross-sectional study conducted by George et al. in Karnataka, only 16.1% of patients with type 2 diabetes were aware of the HbA1c test and its clinical significance. This finding highlights a substantial gap in patient education regarding long-term glycaemic monitoring. Limited awareness of the importance of HbA1c testing may reduce adherence to regular testing schedules and impair timely therapeutic adjustments. Consequently, such gaps in knowledge are likely to contribute to suboptimal disease monitoring, delayed diagnosis, and inadequate treatment intensification, often resulting in persistently elevated HbA1c levels at presentation and during follow-up.
| [13] | George NG, Kamath MS, K MC, Kolar R. HbA1c test awareness, sociodemographic characteristics and lifestyle behaviour among type 2 diabetes mellitus patients. International J Res Med Sci. 2025; 13(12): 5249–54.
https://doi.org/10.18203/2320-6012.ijrms20253945 |
[13]
Many survey respondents perceived sulfonylureas to provide greater glycemic durability in routine clinical practice. This perception aligns with their long-standing role in the management of T2DM. As highlighted by Al-Saleh et al., since their introduction into clinical use in the mid-twentieth century, sulfonylureas have remained an important therapeutic option for T2DM. Their glucose-lowering efficacy is well established, particularly in improving short- to medium-term glycemic control. However, despite their sustained clinical use, there is no clear global consensus across contemporary guidelines regarding the prioritization of sulfonylureas relative to newer antidiabetic therapies. This is largely attributable to limited evidence demonstrating a reduction in macrovascular events or overall mortality compared with some newer drug classes.
| [14] | Al-Saleh Y, Sabico S, Al-Furqani A, Jayyousi A, Alromaihi D, Ba-Essa E, et al. Sulfonylureas in the Current Practice of Type 2 Diabetes Management: Are They All the Same? Consensus from the Gulf Cooperation Council (GCC) Countries Advisory Board on Sulfonylureas. Diabetes Ther. 2021; 12(8): 2115–32. https://doi.org/10.1007/s13300-021-01059-1 |
[14]
Many participants cited multiple factors, namely rapid and sustained glycemic control, reduced pill burden, and cost considerations, as reasons for the early initiation of combination therapy. Phung et al., in a systematic review and meta-analysis of randomized trials, demonstrated that initial combination therapy consistently produced greater reductions in HbA1c and fasting plasma glucose compared with metformin monotherapy, indicating that early use of combination regimens can achieve faster and more durable glycemic control.
| [15] | Phung OJ, Sobieraj DM, Engel SS, Rajpathak SN. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obes Metab. 2014; 16(5): 410–7. https://doi.org/10.1111/dom.12233 |
[15]
Blonde et al. reported that current clinical guidelines and expert opinion support the consideration of initial dual therapy when monotherapy is unlikely to achieve glycemic targets, particularly in patients presenting with elevated HbA1c levels. This aligns with clinician preferences for early combination strategies to reduce prolonged hyperglycemia and the risk of complications.
Hington et al. highlighted fixed-dose or single-pill combination therapy as a promising approach to improve adherence by simplifying treatment regimens and reducing pill burden while maintaining the bioavailability of individual agents. Although early combination therapy may have higher upfront costs,
| [17] | Highton PJ, Funnell MP, Gupta P, Zaccardi F, Lim LL, Seidu S, et al. Improving medication adherence in type 2 diabetes: strategies for better clinical and economic outcomes. Diabetologia. 2026; 69(3): 541–56.
https://doi.org/10.1007/s00125-025-06617-x |
[17]
Ji et al. noted that FDC may be cost-effective over time due to improved glycemic control, fewer complications, and lower overall healthcare utilization, with some economic models favoring first-line combination therapy over stepwise treatment escalation.
| [18] | Ji L, Chan JCN, Yu M, Yoon KH, Kim SG, Choi SH, et al. Early combination versus initial metformin monotherapy in the management of newly diagnosed type 2 diabetes: An East Asian perspective. Diabetes Obes Metab. 2021; 23(1): 3–17.
https://doi.org/10.1111/dom.14205 |
[18]
A majority of clinicians in the current survey reported that individuals with high baseline HbA1c levels (8–11%) derive the greatest benefit from the FDCs of dapagliflozin, glimepiride, and metformin. Supporting this observation, Kurmi et al. reported that patients in the HbA1c 9–11% subgroup (n = 251) demonstrated significantly greater reductions in HbA1c at week 16 with triple FDC therapy (−2.15% and −2.06%) compared with dual therapy (−1.42% and −1.44%), with between-group differences of 0.73% and 0.62% (both p < 0.0001). A higher proportion of patients receiving triple FDC therapy achieved HbA1c <7% (52.7–61.9%) compared with those receiving dual therapy (29.7–43.5%; p < 0.05).
| [19] | Kurmi P, Singh M, Gupta V, Siddegowda C, Shukla J, Gofne S, et al. Subgroup analysis of phase 3 study of fixed-dose combination of dapagliflozin, glimepiride and metformin IR in type 2 diabetes mellitus patients with HbA1c 9%–11%. Endocrine Abstracts. 2024; 99: P 471. |
[19]
Similarly, Zekry et al. reported that both glimepiride and dapagliflozin significantly improved glycemic control and homeostatic model assessment of insulin resistance (HOMA-IR), with no significant difference observed between the two agents. Both drugs were also associated with significant reductions in N-terminal pro–B-type natriuretic peptide levels.
| [20] | Zekry R, Omran GA, El-Gharbawy NM, Werida RH. Comparative study of Dapagliflozin versus Glimepiride effect on insulin regulated aminopeptidase (IRAP) and interleukin-34 (IL-34) in patient with type 2 diabetes mellitus. Sci Rep. 2023; 13(1): 6302. https://doi.org/10.1038/s41598-023-33417-3 |
[20]
Many participants reported that product quality is the most important factor when selecting a brand for the management of T2DM in clinical practice. Fischer et al. emphasized that recognizing individual sensitivities to treatment-related risks and benefits is essential for tailoring effective T2DM management strategies. Their findings help bridge clinical outcomes with patient perspectives, providing useful insights for routine clinical practice, considerations within health technology assessment processes, and the design of clinical studies.
| [21] | Fischer AK, Sadler A, Mathey E, Mühlbacher A. Analysis of patients preferences in type 2 diabetes mellitus second-line drug treatment: A discrete choice experiment. PLoS One. 2025; 20(9): e0329743.
https://doi.org/10.1371/journal.pone.0329743 |
[21]
Mansfield et al. further noted that, given the wide range of therapeutic options currently available for T2DM, engaging patients in discussions about their preferences may improve satisfaction with treatment and support more patient-centered care.
| [22] | Mansfield C, Sikirica MV, Pugh A, Poulos CM, Unmuessig V, Morano R, et al. Patient Preferences for Attributes of Type 2 Diabetes Mellitus Medications in Germany and Spain: An Online Discrete-Choice Experiment Survey. Diabetes Ther. 2017; 8(6): 1365–78. https://doi.org/10.1007/s13300-017-0326-8 |
[22]
The majority of participants reported routinely monitoring patients with T2DM for potential adverse effects or complications. Maureen I. Harris observed that the increase in the frequency of self-monitoring of blood glucose (SMBG) with rising HbA1c levels was largely attributable to a higher proportion of insulin-treated patients within the higher HbA1c categories. However, within specific diabetes therapy groups, the frequency of SMBG was not directly associated with glycemic control as measured by HbA1c.
| [23] | Harris MI, National Health and Nutrition Examination Survey (NHANES III). Frequency of blood glucose monitoring in relation to glycemic control in patients with type 2 diabetes. Diabetes Care. 2001; 24(6): 979–82.
https://doi.org/10.2337/diacare.24.6.979 |
[23]
Jamal et al. highlighted that diabetes self-management programs can effectively incorporate digital technologies into training sessions, and that improved digital literacy and the application of digital health tools may enhance SMBG practices, potentially contributing to better glycemic control in routine care.
| [24] | Jamal A, Tharkar S, Babaier WS, Alsomali SF, Alsulayhim AS, Alayuni MA, et al. Blood Glucose Monitoring and Sharing Amongst People With Diabetes and Their Facilitators: Cross-sectional Study of Methods and Practices. JMIR Diabetes. 2021; 6(4): e29178. https://doi.org/10.2196/29178 |
[24]
Half of the survey participants rated glycemic control with glimepiride as demonstrating marked improvement in routine clinical practice on the 5-point global improvement scale. See et al. reported that glimepiride effectively lowers blood glucose with minimal effects on fasting insulin and body weight, acting via insulin secretion and extrapancreatic mechanisms, reducing hyperinsulinemia‑related risks.
| [25] | See TT, Lee SP, Chen HF, Lee HY. The effect of glimepiride on glycemic control and fasting insulin levels. Journal of Food and Drug Analysis. 2003; 11: 1–3.
https://doi.org/10.38212/2224-6614.2725 |
[25]
Similarly, Schade et al., in a placebo-controlled trial of glimepiride in patients with T2DM unresponsive to dietary measures, reported significant improvements in fasting plasma glucose, HbA1c, and postprandial glucose compared with placebo. Glycemic targets were achieved by 69% of patients receiving glimepiride versus 32% with placebo, with comparable adverse event rates and no clinically meaningful increase in hypoglycemia.
| [26] | Schade DS, Jovanovic L, Schneider J. A placebo-controlled, randomized study of glimepiride in patients with type 2 diabetes mellitus for whom diet therapy is unsuccessful. J Clin Pharmacol. 1998; 38(7): 636–41.
https://doi.org/10.1002/j.1552-4604.1998.tb04471.x |
[26]
A major strength of this nationwide clinician survey (n = 1,300) is its large and geographically diverse sample, which enables comprehensive capture of experts' perspectives on the determinants of poor glycemic control, gaps in early screening, therapeutic preferences, safety considerations, and perceived outcomes associated with contemporary FDCs in T2DM management. The survey offers pragmatic insights into routine clinical practice patterns, including early combination therapy, perceptions of glycemic durability, and monitoring behaviors. However, the findings should be interpreted in light of certain limitations. The self-reported, cross-sectional design introduces the potential for recall, response, and social desirability bias and precludes causal inference. Furthermore, the absence of patient-level clinical data and objective outcome verification limits the ability to directly correlate clinician perceptions with actual glycemic outcomes and may affect the broader generalizability of the results. Although the questionnaire underwent expert review along with face and content validity assessment, quantitative psychometric validation parameters such as Cronbach’s alpha and split-half reliability coefficients were not formally calculated during the study. Therefore, detailed reliability and validity statistics were not available, which may be considered a limitation of the study.
5. Conclusions
This survey highlights key drivers of uncontrolled T2DM, notably sedentary lifestyle, poor follow-up, and low awareness of early screening, which contribute to high baseline HbA1c levels at diagnosis. Clinicians favor sulfonylureas for glycemic durability and frequently select them as add-on therapy to metformin. Early combination therapy is preferred to achieve rapid and sustained glycemic control while reducing pill burden and costs, and FDCs are perceived to delay insulin initiation. Patients with higher baseline HbA1c levels derive the greatest benefit from the dapagliflozin + glimepiride + metformin regimen. Regular monitoring practices, favorable safety perceptions, and meaningful glycemic improvement further support its practical utility in routine clinical care.
Abbreviations
T2DM | Type 2 Diabetes Mellitus |
FDCs | Fixed-Dose Combinations |
HbA1c | Glycated Hemoglobin |
ICMR | Indian Council of Medical Research |
SGLT2 | Sodium-Glucose Cotransporter 2 |
ATP | Adenosine Triphosphate |
ER | Extended Release |
CVOT | Cardiovascular Outcomes Trial |
DPP-4i | Dipeptidyl Peptidase-4 Inhibitors |
SMBG | Self-Monitoring of Blood Glucose |
HOMA-IR | Homeostatic Model Assessment of Insulin Resistance |
FPG | Fasting Plasma Glucose |
ASCVD | Atherosclerotic Cardiovascular Disease |
n | Number of Participants |
p | Probability Value |
SD | Standard Deviation |
CV | Cardiovascular |
ADR | Adverse Drug Reaction |
Author Contributions
Manjula Suresh: Conceptualization, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing
Krishna Kumar Manjunath: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Al-Rifai RH, Aziz F. Prevalence of type 2 diabetes, prediabetes, and gestational diabetes mellitus in women of childbearing age in Middle East and North Africa, 2000-2017: protocol for two systematic reviews and meta-analyses. Syst Rev. 2018; 7(1): 96.
https://doi.org/10.1186/s13643-018-0763-0
|
| [2] |
Yan S, Lu W, Zhou J, Guo X, Li J, Cheng H, et al. Aqueous extract of Scrophularia ningpoensis improves insulin sensitivity through AMPK-mediated inhibition of the NLRP3 inflammasome. Phytomedicine. 2022; 104: 154308.
https://doi.org/10.1016/j.phymed.2022.154308
|
| [3] |
Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health. 2020; 10(1): 107–11.
https://doi.org/10.2991/jegh.k.191028.001
|
| [4] |
Dixit JV, Kulkarni RS, Badgujar SY. Diabetes Care in India: A Descriptive Study. Indian J Endocrinol Metab. 2021; 25(4): 342–7.
https://doi.org/10.4103/ijem.ijem_260_21
|
| [5] |
Chinese Endocrinologist Association. [Expert consensus on combination therapies of oral anti-diabetic drugs for adults with type 2 diabetes (2025 edition)]. Zhonghua Nei Ke Za Zhi. 2025; 64(8): 707–22.
https://doi.org/10.3760/cma.j.cn112138-20250515-00279
|
| [6] |
Sahay R, Gangwani D, Singh M, Gupta S, Kale N, Srivastava M, et al. Fixed dose combination of dapagliflozin, glimepiride and extended-release metformin tablets in patients with type 2 diabetes poorly controlled by metformin and glimepiride: A phase III, open label, randomized clinical study in India. Diabetes Obes Metab. 2025; 27(4): 2193–205.
https://doi.org/10.1111/dom.16218
|
| [7] |
Dhillon S. Dapagliflozin: A Review in Type 2 Diabetes. Drugs. 2019; 79(10): 1135-1146.
https://doi.org/10.1007/s40265-019-01148-3
|
| [8] |
Basit A, Riaz M, Fawwad A. Glimepiride: evidence-based facts, trends, and observations (GIFTS). Vasc Health Risk Manag. 2012; 8: 463-72.
https://doi.org/10.2147/HIV.S33194
|
| [9] |
Dutta S, Shah RB, Singhal S, Dutta SB, Bansal S, Sinha S, et al. Metformin: A Review of Potential Mechanism and Therapeutic Utility Beyond Diabetes. Drug Des Devel Ther. 2023; 17: 1907-1932.
https://doi.org/10.2147/DDDT.S409373
|
| [10] |
Damayanti LS. The impact of sedentary behavior on blood glucose levels in type 2 diabetes mellitus patients: A literature review. Journal of Evidence-based Nursing and Public Health. 2025; 2(1): 34–52.
https://doi.org/10.61511/jevnah.v2i1.2025.1735
|
| [11] |
Bellettiere J, Healy GN, LaMonte MJ, Kerr J, Evenson KR, Rillamas-Sun E, et al. Sedentary Behavior and Prevalent Diabetes in 6,166 Older Women: The Objective Physical Activity and Cardiovascular Health Study. J Gerontol A Biol Sci Med Sci. 2019; 74(3): 387–95.
https://doi.org/10.1093/gerona/gly101
|
| [12] |
Halder U. Diabetes as a pandemic: A sociological study on awareness, negligence and lifestyle at Howrah District. Int J Med Health Res. 2025; 11(6): 8-12.
|
| [13] |
George NG, Kamath MS, K MC, Kolar R. HbA1c test awareness, sociodemographic characteristics and lifestyle behaviour among type 2 diabetes mellitus patients. International J Res Med Sci. 2025; 13(12): 5249–54.
https://doi.org/10.18203/2320-6012.ijrms20253945
|
| [14] |
Al-Saleh Y, Sabico S, Al-Furqani A, Jayyousi A, Alromaihi D, Ba-Essa E, et al. Sulfonylureas in the Current Practice of Type 2 Diabetes Management: Are They All the Same? Consensus from the Gulf Cooperation Council (GCC) Countries Advisory Board on Sulfonylureas. Diabetes Ther. 2021; 12(8): 2115–32.
https://doi.org/10.1007/s13300-021-01059-1
|
| [15] |
Phung OJ, Sobieraj DM, Engel SS, Rajpathak SN. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obes Metab. 2014; 16(5): 410–7.
https://doi.org/10.1111/dom.12233
|
| [16] |
Blonde L, Dipp S, Cadena D. Combination Glucose-Lowering Therapy Plans in T2DM: Case-Based Considerations. Adv Ther. 2018; 35(7): 939–65.
https://doi.org/10.1007/s12325-018-0694-0
|
| [17] |
Highton PJ, Funnell MP, Gupta P, Zaccardi F, Lim LL, Seidu S, et al. Improving medication adherence in type 2 diabetes: strategies for better clinical and economic outcomes. Diabetologia. 2026; 69(3): 541–56.
https://doi.org/10.1007/s00125-025-06617-x
|
| [18] |
Ji L, Chan JCN, Yu M, Yoon KH, Kim SG, Choi SH, et al. Early combination versus initial metformin monotherapy in the management of newly diagnosed type 2 diabetes: An East Asian perspective. Diabetes Obes Metab. 2021; 23(1): 3–17.
https://doi.org/10.1111/dom.14205
|
| [19] |
Kurmi P, Singh M, Gupta V, Siddegowda C, Shukla J, Gofne S, et al. Subgroup analysis of phase 3 study of fixed-dose combination of dapagliflozin, glimepiride and metformin IR in type 2 diabetes mellitus patients with HbA1c 9%–11%. Endocrine Abstracts. 2024; 99: P 471.
|
| [20] |
Zekry R, Omran GA, El-Gharbawy NM, Werida RH. Comparative study of Dapagliflozin versus Glimepiride effect on insulin regulated aminopeptidase (IRAP) and interleukin-34 (IL-34) in patient with type 2 diabetes mellitus. Sci Rep. 2023; 13(1): 6302.
https://doi.org/10.1038/s41598-023-33417-3
|
| [21] |
Fischer AK, Sadler A, Mathey E, Mühlbacher A. Analysis of patients preferences in type 2 diabetes mellitus second-line drug treatment: A discrete choice experiment. PLoS One. 2025; 20(9): e0329743.
https://doi.org/10.1371/journal.pone.0329743
|
| [22] |
Mansfield C, Sikirica MV, Pugh A, Poulos CM, Unmuessig V, Morano R, et al. Patient Preferences for Attributes of Type 2 Diabetes Mellitus Medications in Germany and Spain: An Online Discrete-Choice Experiment Survey. Diabetes Ther. 2017; 8(6): 1365–78.
https://doi.org/10.1007/s13300-017-0326-8
|
| [23] |
Harris MI, National Health and Nutrition Examination Survey (NHANES III). Frequency of blood glucose monitoring in relation to glycemic control in patients with type 2 diabetes. Diabetes Care. 2001; 24(6): 979–82.
https://doi.org/10.2337/diacare.24.6.979
|
| [24] |
Jamal A, Tharkar S, Babaier WS, Alsomali SF, Alsulayhim AS, Alayuni MA, et al. Blood Glucose Monitoring and Sharing Amongst People With Diabetes and Their Facilitators: Cross-sectional Study of Methods and Practices. JMIR Diabetes. 2021; 6(4): e29178.
https://doi.org/10.2196/29178
|
| [25] |
See TT, Lee SP, Chen HF, Lee HY. The effect of glimepiride on glycemic control and fasting insulin levels. Journal of Food and Drug Analysis. 2003; 11: 1–3.
https://doi.org/10.38212/2224-6614.2725
|
| [26] |
Schade DS, Jovanovic L, Schneider J. A placebo-controlled, randomized study of glimepiride in patients with type 2 diabetes mellitus for whom diet therapy is unsuccessful. J Clin Pharmacol. 1998; 38(7): 636–41.
https://doi.org/10.1002/j.1552-4604.1998.tb04471.x
|
Cite This Article
-
APA Style
Suresh, M., Manjunath, K. K. (2026). Clinicians' Perspectives on Glycemic Control, Treatment Strategies, and Monitoring in Type 2 Diabetes Mellitus:
A Nationwide Survey. International Journal of Diabetes and Endocrinology, 11(2), 20-27. https://doi.org/10.11648/j.ijde.20261102.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Suresh, M.; Manjunath, K. K. Clinicians' Perspectives on Glycemic Control, Treatment Strategies, and Monitoring in Type 2 Diabetes Mellitus:
A Nationwide Survey. Int. J. Diabetes Endocrinol. 2026, 11(2), 20-27. doi: 10.11648/j.ijde.20261102.12
Copy
|
Download
AMA Style
Suresh M, Manjunath KK. Clinicians' Perspectives on Glycemic Control, Treatment Strategies, and Monitoring in Type 2 Diabetes Mellitus:
A Nationwide Survey. Int J Diabetes Endocrinol. 2026;11(2):20-27. doi: 10.11648/j.ijde.20261102.12
Copy
|
Download
-
@article{10.11648/j.ijde.20261102.12,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Clinicians' Perspectives on Glycemic Control, Treatment Strategies, and Monitoring in Type 2 Diabetes Mellitus:
A Nationwide Survey},
journal = {International Journal of Diabetes and Endocrinology},
volume = {11},
number = {2},
pages = {20-27},
doi = {10.11648/j.ijde.20261102.12},
url = {https://doi.org/10.11648/j.ijde.20261102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijde.20261102.12},
abstract = {Background: Although there are several clinical studies available regarding the management of Type 2 diabetes mellitus (T2DM), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the drivers of poor glycemic control, gaps in early screening, treatment choices, use of fixed-dose combinations (FDCs) of dapagliflozin, glimepiride, and metformin, safety considerations, and perceived glycemic outcomes in T2DM. Methodology: This cross-sectional study was carried out among 1,300 Indian clinical experts and utilized a multiple-response questionnaire to assess perspectives on poor glycemic control, screening gaps, and treatment patterns related to FDCs of dapagliflozin, glimepiride, and metformin. Responses were summarized using descriptive statistics and visualized using Microsoft Excel. Results: More than half of the participants (54.46%) identified a sedentary lifestyle and irregular follow-up visits as the principal contributors to poor glycemic control in routine clinical practice. A substantial majority (68.77%) indicated that inadequate awareness of early screening is the primary reason for elevated glycated hemoglobin (HbA1c) levels at diagnosis. Over half of the respondents (52.23%) perceived sulfonylureas to provide superior glycemic durability in clinical settings. Approximately 42% reported multiple factors, namely rapid and sustained glycemic control, reduced pill burden, and cost considerations, as key reasons for the early initiation of combination therapy. Nearly two-thirds of clinicians (63.46%) observed that patients with high baseline HbA1c levels (8–11%) experience the greatest benefit from the FDCs of dapagliflozin, glimepiride, and metformin. Conclusion: Uncontrolled T2DM is primarily driven by a sedentary lifestyle, poor follow-up, and low awareness of early screening. Clinicians favor sulfonylureas for glycemic durability and support early combination therapy for rapid control, improved adherence, and cost considerations. FDCs are perceived to delay insulin initiation, with patients presenting with high baseline HbA1c levels deriving the greatest benefit from the combination of dapagliflozin, glimepiride, and metformin.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinicians' Perspectives on Glycemic Control, Treatment Strategies, and Monitoring in Type 2 Diabetes Mellitus:
A Nationwide Survey
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/27
PY - 2026
N1 - https://doi.org/10.11648/j.ijde.20261102.12
DO - 10.11648/j.ijde.20261102.12
T2 - International Journal of Diabetes and Endocrinology
JF - International Journal of Diabetes and Endocrinology
JO - International Journal of Diabetes and Endocrinology
SP - 20
EP - 27
PB - Science Publishing Group
SN - 2640-1371
UR - https://doi.org/10.11648/j.ijde.20261102.12
AB - Background: Although there are several clinical studies available regarding the management of Type 2 diabetes mellitus (T2DM), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the drivers of poor glycemic control, gaps in early screening, treatment choices, use of fixed-dose combinations (FDCs) of dapagliflozin, glimepiride, and metformin, safety considerations, and perceived glycemic outcomes in T2DM. Methodology: This cross-sectional study was carried out among 1,300 Indian clinical experts and utilized a multiple-response questionnaire to assess perspectives on poor glycemic control, screening gaps, and treatment patterns related to FDCs of dapagliflozin, glimepiride, and metformin. Responses were summarized using descriptive statistics and visualized using Microsoft Excel. Results: More than half of the participants (54.46%) identified a sedentary lifestyle and irregular follow-up visits as the principal contributors to poor glycemic control in routine clinical practice. A substantial majority (68.77%) indicated that inadequate awareness of early screening is the primary reason for elevated glycated hemoglobin (HbA1c) levels at diagnosis. Over half of the respondents (52.23%) perceived sulfonylureas to provide superior glycemic durability in clinical settings. Approximately 42% reported multiple factors, namely rapid and sustained glycemic control, reduced pill burden, and cost considerations, as key reasons for the early initiation of combination therapy. Nearly two-thirds of clinicians (63.46%) observed that patients with high baseline HbA1c levels (8–11%) experience the greatest benefit from the FDCs of dapagliflozin, glimepiride, and metformin. Conclusion: Uncontrolled T2DM is primarily driven by a sedentary lifestyle, poor follow-up, and low awareness of early screening. Clinicians favor sulfonylureas for glycemic durability and support early combination therapy for rapid control, improved adherence, and cost considerations. FDCs are perceived to delay insulin initiation, with patients presenting with high baseline HbA1c levels deriving the greatest benefit from the combination of dapagliflozin, glimepiride, and metformin.
VL - 11
IS - 2
ER -
Copy
|
Download